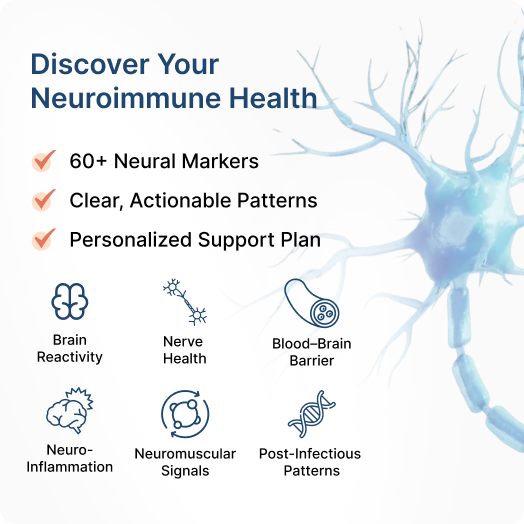
Neural Zoomer offers a clear, clinically meaningful view of how immune activity may be influencing your brain and nervous system. By measuring antibodies tied to neuroinflammation, brain and nerve structures, and blood–brain barrier balance, it brings structure to complex neurological symptoms and supports more informed, personalized care for long-term brain clarity and resilience.
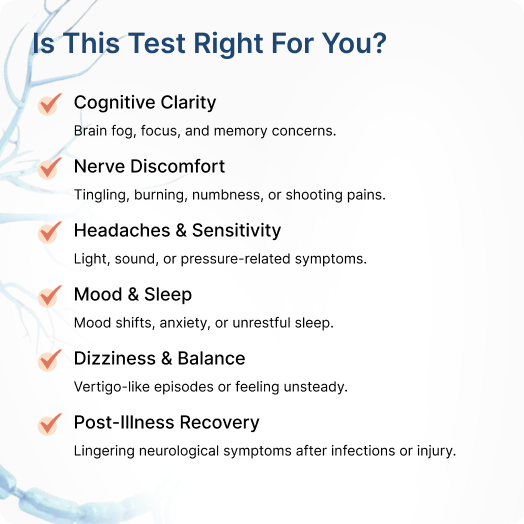


The myelin sheath helps your nerves send clear, steady signals. When the immune system interacts with myelin proteins, it may relate to symptoms such as tingling, weakness, or balance changes.
Precision Testing
Measures immune responses to MOG, MAG, MBP, PLP, tubulin, and neurofascin, key proteins that support nerve insulation.
Personalized Insights
Focuses on nutrients, lifestyle habits, and nervous-system practices that help maintain myelin integrity and smooth nerve communication.










.png?width=835&height=831&name=Screenshot%202025-09-05%20at%2016.11.51%201%20(1).png)
.png?width=834&height=828&name=Screenshot%202025-09-05%20at%2016.11.51%201%20(3).png)
.png?width=835&height=828&name=Screenshot%202025-09-05%20at%2016.11.51%201%20(4).png)


.png?width=457&height=457&name=Step%20Images%20(1).png)


.png?width=900&height=735&name=image%20859%20(1).png)